
Emotions attached to this venture are to provide customized, suitable and affordable hearing solutions. Highly qualified professionals for your treatments
Our USP is that we are multi brand clinic with highly qualified and experienced Audiologist and speech language pathologists. Patient’s benefit is our top concern
(PTA) is the key hearing test used to identify hearing threshold levels of an individual, enabling determination of the degree, type and configuration of a hearing loss and thus providing a basis for diagnosis and management.
This type of testing is used to measure your speech reception threshold (SRT), or the faintest speech you can understand 50 percent of the time. It is administered in either a quiet or noisy environment and measures your ability to separate speech from background noise.
This test measures the movement of your eardrum in response to air pressure. It can determine if there is a buildup of fluid, wax buildup, eardrum perforations or tumors.
This test measures involuntary muscle contractions of the middle ear and is used to determine the location of your hearing problem (the ossicles, cochlea, auditory nerve, etc.) as well as the type of hearing loss.
This type of testing is used to determine whether a specific type of hearing loss—sensorineural—exists. It is also frequently used to screen newborns for hearing problems. In an ABR test, electrodes are attached to your head, scalp or earlobes, and you are given headphones to wear. Your brainwave activity is measured in response to sounds of varying intensities.
OAEs are sounds generated by the vibrations of the hair cells in the cochlea of your inner ear. This type of testing uses a tiny uses probe fitted with a microphone and speaker to stimulate the cochlea and measure its response. Individuals with normal hearing will produce emissions; when hearing loss exceeds 25-30 decibels, no sound will be produced. This test helps determine whether there is a blockage in the ear canal, excess fluid in the middle ear or damage to the hair cells of the cochlea. OAE testing is often included in newborn hearing screening programs.

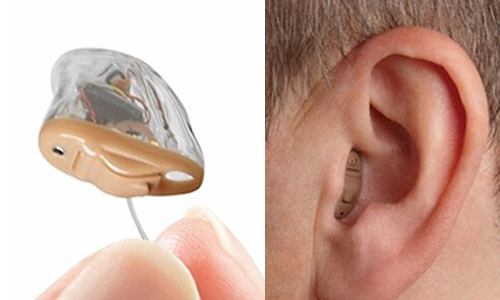
This custom-fitted style is inserted farther into the ear canal than other styles, so it’s completely invisible* when worn. IIC hearing aids are designed to be removed daily to promote good ear health. For mild to moderate hearing loss. *Individual results may vary. Invisibility may vary based on your ear’s anatomy.
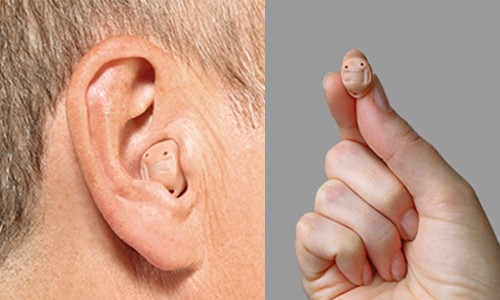
CIC hearing instruments are custom-made to fit completely in the ear canal. Only the tip of a small plastic “handle” shows outside the canal, which is used to insert and remove the instrument. For mild to moderate hearing loss.
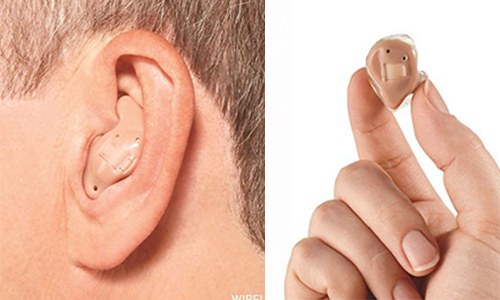
ITC hearing instruments are custom-made to fit in the ear canal with a smaller portion of the hearing aid showing in the outer ear. For mild to mildly severe hearing loss.
ITE hearing instruments are custom-made to fit within the outer portion of the ear. For mild to severe hearing loss.

Barely visible when worn, the RIC style is an instrument in which the receiver, or speaker, is inside the ear canal. Thin electrical wires are used instead of a plastic acoustical tube, reducing distortion.RIC hearing aids provide a comfortable, open fit. For mild to moderate hearing loss.

The hearing technology is housed in a casing that rests behind the ear. A clear plastic acoustical tube directs amplified sound into an earbud or a customized earmold that is fitted inside the ear canal. For moderate to severe hearing loss.
Cochlear implants are surgically implanted devices that provide electrical stimulation to the auditory system, which is perceived within the brain as sound.
A cochlear implant is a surgically placed device that helps a person with severe hearing loss hear sounds.
The cochlea is a snail-shaped part of the inner ear. It turns sound vibrations into electrical signals that travel along the auditory (hearing) nerve. The brain translates these signals into recognizable sounds.
Cochlear (KOE-klee-er) implants are different from hearing aids:
Cochlear implants have:
Doctors consider cochlear implants for children under 12 months of age with profound hearing loss in both ears. Older children with serious hearing loss also may get cochlear implants.
A cochlear implant team will help decide if cochlear implants are a good option. This team includes an audiologist (hearing specialist), an ear-nose-throat (ENT) doctor, a speech therapist, a psychologist, and a social worker.
Kids being considered for the surgery will:
Kids might not get the implants if:
As has often been said, children are not “little adults.” They are indeed, unique, and to address their CI needs, they require an experienced clinician. Most children are unable to provide accurate feedback while the audiologist programs their cochlear implant and therefore, the clinician must take many things into account:
Many of the decisions made during programming appointments come from the clinician’s knowledge and experience, rather than the child’s behavioral responses
Although cochlear implant maps are individualized and set according to the patient’s physiologic responses, there are trends witnessed across patient populations.
(As stated above, T level (threshold) is the least amount of electrical current necessary for a person to perceive a sound. The C or M level is the most comfortable level, or a loud but comfortable level. The CI dynamic range is defined as the difference between T and C/M levels These parameters are referred to as the patient’s “map.”)
With the Cochlear Americas Nucleus 24 device, the amount of electrical stimulation available (using default programming parameters) is between 0 and 240 clinical units (cus) and it is extremely rare to see T levels at or below 100 cus. Additionally, there are not many adult patients that have C levels above 210 cus. With the Advanced Bionics HiRes processing strategy, average M levels are between 100 cus and 300cus. More information on average stimulation levels can be found in Zwolan & Overstreet [9].
Etiology of hearing loss also appears to influence stimulation levels, possibly due to neural survival. For example, a patient deafened from meningitis may have extremely high stimulation levels, while a patient with Connexin 26 gene deficits may have extremely low stimulation levels.
When a patient’s device is initially activated, stimulation levels change frequently while the patient is learning to listen with their cochlear implant. Figure A shows how cochlear implant maps change over the first two years, as was determined on post-lingually deafened adult. As the graph shows, stimulation levels increased during the beginning of her CI experience, but eventually a plateau was seen and stimulation levels hovered in a certain clinical unit range.
One theory as to why this phenomenon exists could be — At first, the auditory system is extremely sensitive to the electrical stimulus and is learning how to manage the information. After continued use and practice, the brain adjusts (neural plasticity) and learns to effectively use the electrical input. Over time, the person requires higher stimulation levels to hear optimally, and the parameters that become the optimal map generally remain stable for many years of cochlear implant use. It is important to note that the majority of adult CI users do not have stimulation levels that continue to increase over time. If they did, the patient would eventually reach the output limits of the device and no longer benefit from their cochlear implant.
It appears that pediatric maps show higher stimulation levels over time, as compared to adult cochlear implant maps[10]. Researchers hypothesize that children will often adapt to their program settings, even if they are set too high, and therefore, gradual increases in stimulation at subsequent programming visits may not be necessary. Additionally, Overstreet et al found that adults with lower stimulation levels performed better on speech perception tasks. Additionally, negative effects from high stimulation levels exist, including; risk of facial nerve stimulation, increased channel interaction, low battery life, voltage compliance issues and may result in an eventual degradation of the speech signal.
Overstimulation (“overstim”) is the term used to describe cochlear implant map settings with stimulation levels exceeding the amount needed to create the desired percept. Overstim can occur due to a lack of patient participation, pressure from the parents/therapists, and/or inappropriate or inaccurate implementation of objective measures. When stimulation levels are set too high, sound quality and auditory skills can be affected.
Adult patients have previously described how changes in their map impacts their listening experience. If threshold levels are set too high, soft sounds are perceived as loud. For example, a light tapping sound could be perceived as a loud knocking sound, and in effect, consonant sounds could be heavily distorted. Although children may overcome the difficulty in perceiving and distinguishing between consonant sounds when they are distorted in this manner, the child may exhibit poor speech production skills since they are producing the sounds as they are hearing them. Overstim might also exasperate background noise, resulting in poorer listening abilities in noise.
Adult patients have sometimes caused their own overstim by falsely assuming that setting their comfort levels louder results in clearer sound, when in fact, the opposite occurs. When C/M levels are too high, patients describe experiencing echoing, bubbly, or wavering sounds. However, these subjective descriptions can also exist when a person’s comfort levels are set too low. Therefore, the patient may have to listen to a variety of sounds and comfort levels to determine the best map for them.
It is clear that focused and accurate participation during cochlear implant programming is the preferred route to creating an optimal map. However, children cannot usually provide such information due to their current language abilities and the complex nature of discussing concepts of loudness and sound quality. Difficulty expressing their CI experience paired with unreliable behavioral information (due to lack of participation, attention problems or poor behavior) can lead to map settings that are inappropriate. Therefore, case studies are offered here (below) to demonstrate the effects of overstimulation.
Speech-language therapy is the treatment for most kids with speech and/or language disorders.
A speech disorder refers to a problem with making sounds. Speech disorders include:
A language disorder refers to a problem understanding or putting words together to communicate ideas. Language disorders can be either receptive or expressive:
Dysphagia/oral feeding disorders are disorders in the way someone eats or drinks. They include problems with chewing and swallowing, coughing, gagging, and refusing foods.
Speech-language pathologists (SLPs), often called speech therapists, are educated in the study of human communication, its development, and its disorders. SLPs assess speech, language, cognitive-communication, and oral/feeding/swallowing skills. This lets them identify a problem and the best way to treat it.
Sometimes, speech assistants help give speech-language services. They usually have a 2-year associate’s or 4-year bachelor’s degree, and are supervised by an SLP.
In speech-language therapy, an SLP works with a child one-on-one, in a small group, or in a classroom to overcome problems.
Kids might need speech-language therapy for many reasons, including:
Therapy should begin as soon as possible. Children who start therapy early (before they’re 5 years old) tend to have better results than those who begin later.
This doesn’t mean that older kids won’t do well in therapy. Their progress might be slower, though, because they have learned patterns that need to be changed.
To find a specialist, ask your child’s doctor or teacher for a referral, check local directories online, or search on ASHA’s website. State associations for speech-language pathology and audiology also keep listings of licensed and certified therapists.
Your child’s SLP should be licensed in your state and have experience working with kids and your child’s specific disorder.
Parents are key to the success of a child’s progress in speech or language therapy. Kids who finish the program quickest and with the longest-lasting results are those whose parents were involved.
Ask the therapist what you can do. For instance, you can help your child do the at-home activities that the SLP suggests. This ensures the continued progress and carry-over of new skills.

Though hearing assessment or screening for every infant is ideally , it should be done for babies having high risk factors such as:

Preterm Birth.
Low birth weight.
Jaundice/ Hyperbillirubenemia.
Anoxia/ hyperbaric oxygen treatment.
Maternal intrauterine infections such as rubella, toxoplasmosis.
NICU admission for more than 48 hours.
Craniofacial anomalies.
Ototoxic drug.
